On Treating Lyme Disease
Beyond antibiotics, toward a theory of herbal war

I woke up with half my face paralyzed. Sure, I’d been concerned about unrelenting exhaustion for weeks. But I’d just come off a particularly brutal on-call stretch of residency, so it wasn’t totally unexpected. Grueling 24-hour shifts every 4 days, stretches managing the mental health of an entire 500-bed hospital, 2 inpatient psychiatric units, and a chaotic regional emergency department – every night, by myself – from 5pm-8am. Duh, I thought, exhaustion is the price.
But then one morning I tried to swallow a big gulp of water, and it just squirted out of my mouth. WTF? Wait — I can’t close my lips down tight. I can’t close one eye, can’t smile, trouble enunciating. Holy shit, my face is becoming paralyzed. This is a facial nerve palsy. Okay, shit. This is Lyme.
The literature on Lyme facial nerve palsies is not exactly encouraging. “Most achieve complete recovery with in 6 months.” Six months?! Dear god — If this gets any worse I won’t be able to close my eye to sleep, talk normally with patients, or even pass for a normal looking person. And for some it lasts longer?!
So I did what I always do when faced with a health question: drew upon any and everything to chart the path forward — conventional and integrative, a pluralistic epistemological method. The following piece is the framework I developed to treat myself, a combination of conventional and evidence-guided herbalism along with a treatment regimen that, in retrospect, bears some resemblance to the logic of upfront, multi-agent combination chemotherapy. It worked. And I’ve been asked numerous times by numerous friends and friends of friends to share my approach. This was my approach — this is not medical advice, but if god forbid you ever find yourself with runaway Lyme, it may be helpful to see my thought process.
Day of aforementioned palsy: “Smile harder.” / “This is hard as I can! My face is broken!”
Reminder: this is not medical advice. This is general information. Reading this essay does not establish a doctor-patient relationship. Talk to your own clinician before making changes to your health. Use the powerful information below responsibly and at your own risk.
There’s a lot of confusion about Lyme Disease.
To begin with, we have to be able to hold two things simultaneously:
The impacts of Lyme disease are both devastating and under-appreciated—and—it’s also wildly misattributed.
Lyme disease — the devastation it can have — is textbook sneaky, it’s caught far too late, and it can ruin people’s lives. Advanced Lyme disease can kill you, put you in the hospital, debilitate you from walking, thinking, being. There are many public figures who’ve been open about their experiences with serologically confirmed Lyme. It’s awful.
And there’s a lot more going on with what can be called chronic Lyme disease than is often appreciated. This is controversial. Within the conventional evidence base, many deny the concept of chronic Lyme, pointing to studies that demonstrate no evidence of active infection. And yet, if you pay attention to patients, there is obviously something more going on.
I knew this from my days in medical school at Columbia, where I had conversations with one of the leading researchers on this topic. It seems likely that there is a post-infectious illness — akin to something like long COVID — in which the body’s immune regulation, inflammatory set point, etc, become scrambled, leaving people suffering, often profoundly, without clear guidance or treatment. The frontier literature now groups post-treatment Lyme with long COVID, post-EBV ME/CFS, post-Q-fever fatigue, and others under the umbrella of post-acute infection syndromes — sharing immune dysregulation, dysautonomia, and neuroinflammatory features regardless of the triggering pathogen.1
It’s absurd to write this all off as psychosomatic. A Hopkins prospective cohort found ideally-treated Lyme patients were 5.28 times more likely than controls to meet operationalized post-treatment criteria, with eight to fifteen times higher odds of moderate-to-severe fatigue and muscle pain.2
It also seems, to some degree, there are persisting forms of infection. The Lyme spirochete, a cousin of syphilis, is highly adept at immune evasion, with multiple morphologic forms that are very good at hiding from the body.3
Now, the second piece we need to hold:
Lyme attracts snake oil salesmen and charlatans like moths to a lamp.
I’ve seen this firsthand. You’ve got some shady functional or integrative medicine practitioner who attributes any unexplained or systemic illness to Lyme. And, coincidentally, their treatment — costing many thousands of dollars — is something their clinic just so happens to provide.
Be very wary of these folks.
(Note: many functional/integrative practitioners are excellent, some of the best, but the spread is wide and the range of conflict-of-interest-driven charlatans is extraordinary.)
The result of holding both of these truths is a very lonely middle ground: to utilize and consider the robust, conventional evidence based and treatments, while also having the humility to recognize that empirically, there’s a lot more going on here, for many people our approach is not sufficient, and there are extremely cost-benefit favorable treatments we can add on to the conventional approach.
A milligram of prevention is worth an ounce of antibiotics
Before getting into treatment, we do need to say the boring-but-absolutely-true thing: the best Lyme protocol is never needing one. We’ll break this down with a few paragraphs on recognizing risk, preventing exposure, and responding to a high-risk tick bite. If this is familiar territory, feel free to skip down to the Treatment section.
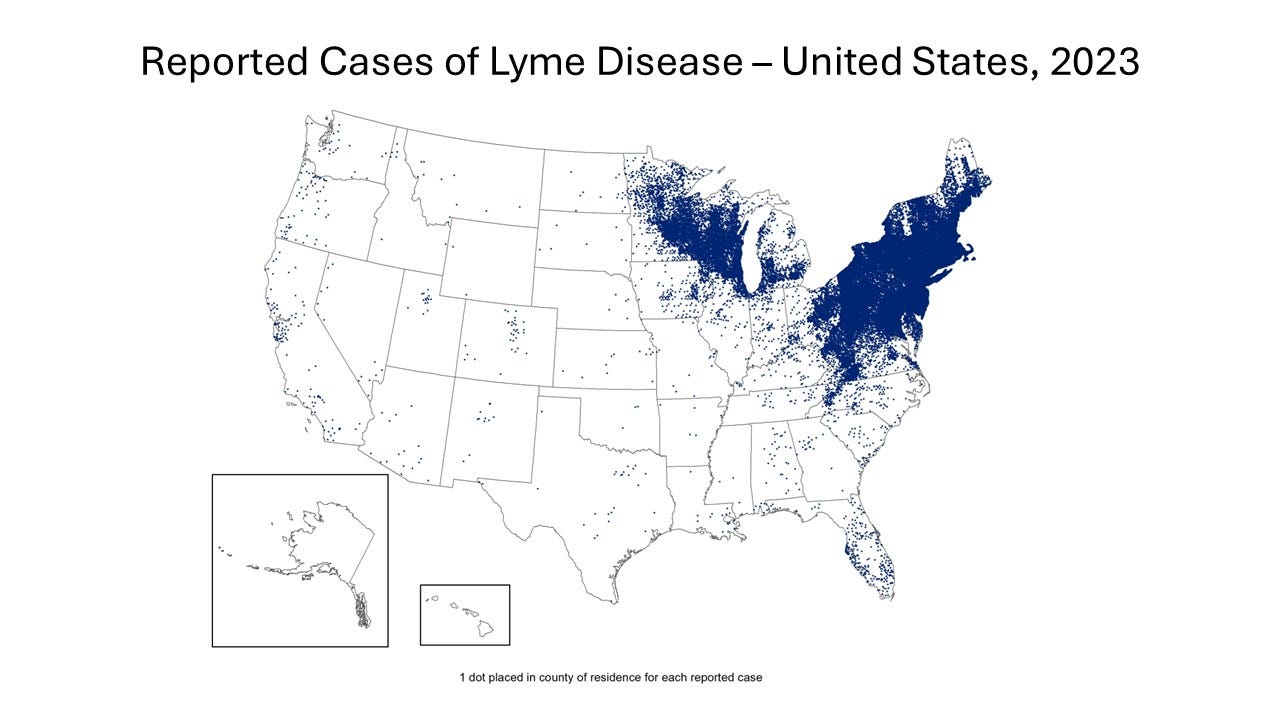
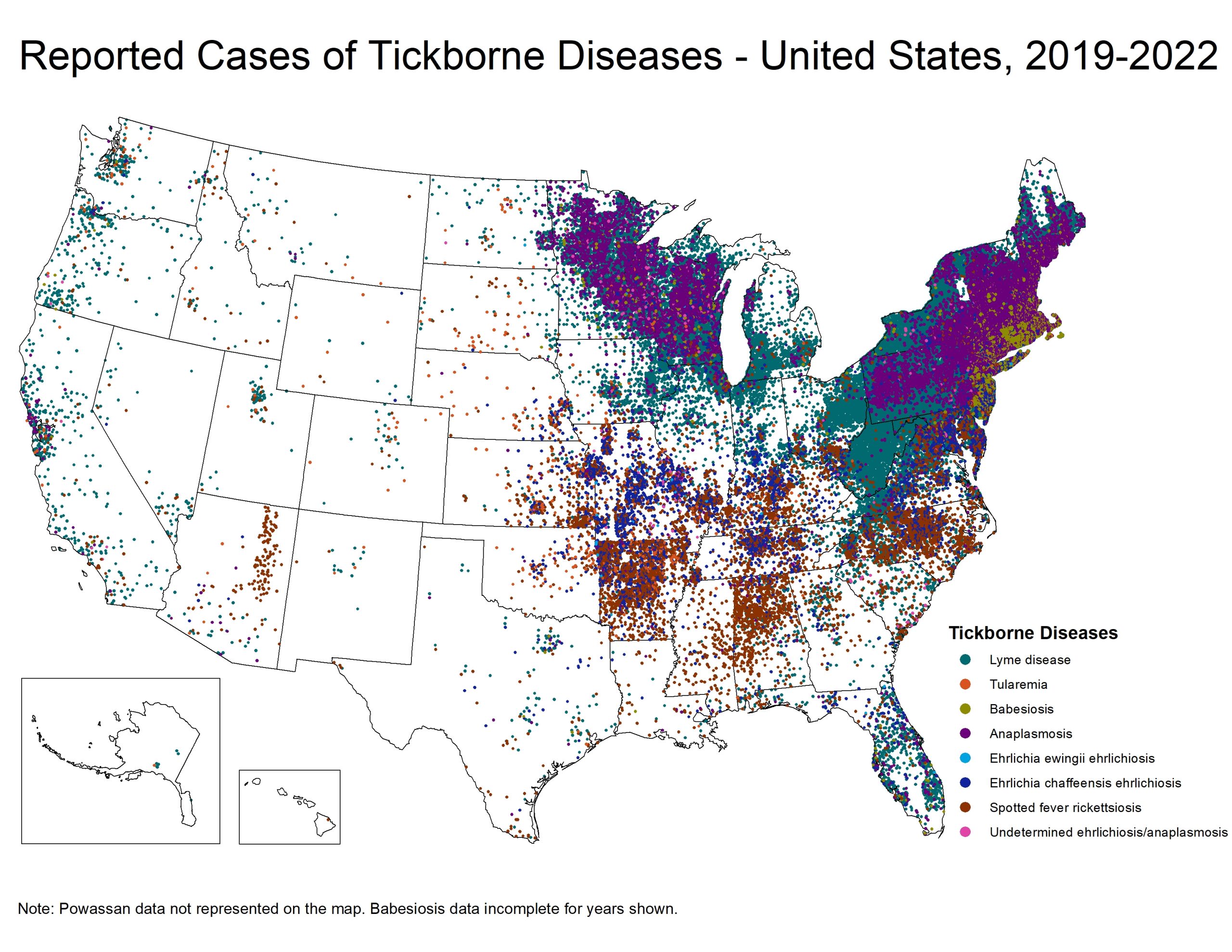
First — know where you’re at risk. Yes, you can contract Lyme in California but it’s a hell of a lot rarer than in Connecticut.
{kind=link}
{kind=link}
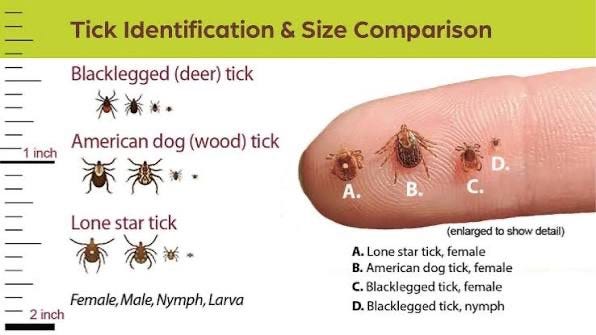
Understand that if you’re in an endemic region, you should be appropriately neurotic about prevention (i.e. proper clothing +/- treated with permethrin) and rigorous with tick checks following time in nature — especially after being in places ticks love: humid, leafy forests, low brush and tall grass, forest edges, overgrown fields, etc. You should be familiar with identifying tick species (see graphic below, see this excellent guide). You may want to have a high quality tick removal tweezer on hand just in case. You can even consider keeping a tick testing kit to send out in the event of finding one engorged so you can see if the deer tick is infected (up to 50% are, depending on region and life cycle). The CDC doesn’t recommend making treatment decisions based on tick testing for sound reasons, but I think it can be a helpful piece of data — see this footnote for more.4
Prophylaxis
Now — let’s say you did or didn’t follow the above, and you’ve found a tick. You should know about prophylaxis. The transmission of Borrelia burgdorferi (the bacterium which causes Lyme disease) requires 36-48 hours of tick attachment in most cases, which will be evident by tick engorgement — see this at the bottom of “Tick ID page 3” for what engorgement looks like. Risk rises the longer the tick stays on and feeds. Even in endemic areas, the per-bite risk is still relatively low in absolute terms, but it grows with prolonged attachment and engorgement. The big problem is that the highest-risk ticks are often nymphs, which are the size of poppy-seeds — extremely difficult to notice!
For this reason, single-dose doxycycline prophylaxis (200 mg for adults) within the 72 hour window of tick removal is recommended by the IDSA/AAN/ACR guidelines for high-risk Ixodes (deer) tick bites. High-risk is defined as meeting all of the following (5) criteria:
(1) Identified Ixodes species tick (deer tick), (2) occurred in a highly endemic area, (3) tick attached ≥36 hours (evidenced by engorgement), (4) removed within 72 hours, and (5) doxycycline is safe for the patient.5
Nearly 75% of deer ticks removed from humans have fed less than 48 hours, so most recognized bites do not meet high-risk criteria. However, unrecognized bites pose greater risk since undetected ticks are more likely to feed for days and thereby balloon transmission risk, and the small size of nymphal ticks (poppy-sized sneaky) and frequent exposure in endemic areas create cumulative risk.6
So let’s say you don’t catch the tick at all. Once Lyme disease is suspected or diagnosed, our approach changes.
Recognize the symptoms of Lyme
You should familiarize yourself with the symptoms of Lyme disease. The CDC has a great visual guide to Lyme rashes and symptom patterns. A common misconception is that Lyme always comes along with the classic bullseye rash. It does not. Erythema migrans (said rash) occurs in ~70% of people with Lyme disease, which means a sizable minority never get the rash at all. If you do see a classic expanding bullseye rash after possible tick exposure, that is highly specific for Lyme. The rash is not always a perfect bullseye. The absence of a rash should not reassure you if the rest of the symptoms fit, which can include some mix of: fever, chills, headache, profound fatigue, muscle/joint aches, swollen lymph nodes, facial palsy, nerve pain, migratory joint pain, and more. Some of these symptoms are specific. Others are incredibly vague and generalized. Lyme disease does weird things. And for that reason it’s always in the back of a physician’s mind when a patient in an endemic region has all sorts of weird and unexplained symptoms that don’t add up.
Antibiotics
Doxycycline as a first-line treatment — especially if you get it early — is extremely effective. It’s the most effective treatment we have, and for most people will eradicate Lyme entirely. You move on with your life. But — roughly 12–15% of patients with early Lyme report persistent fatigue, musculoskeletal pain, or cognitive symptoms at six months post-treatment.7 For early disseminated disease with neurologic involvement (my case), the residuals are more common still — more than half at 4 months, and roughly 28% at last follow-up in a corpus that includes studies tracking patients out to 20 years .89 This is why we employ a pluralistic approach — downside insurance.
Nonetheless, doxycycline works well for most. But it also disrupts your gut microbiome, and those consequences are still extremely under-appreciated. While that’s a nontrivial trade-off, and worth further discussion below, uncontrolled disseminated Lyme disease is much, much worse.
On microbiome disruption
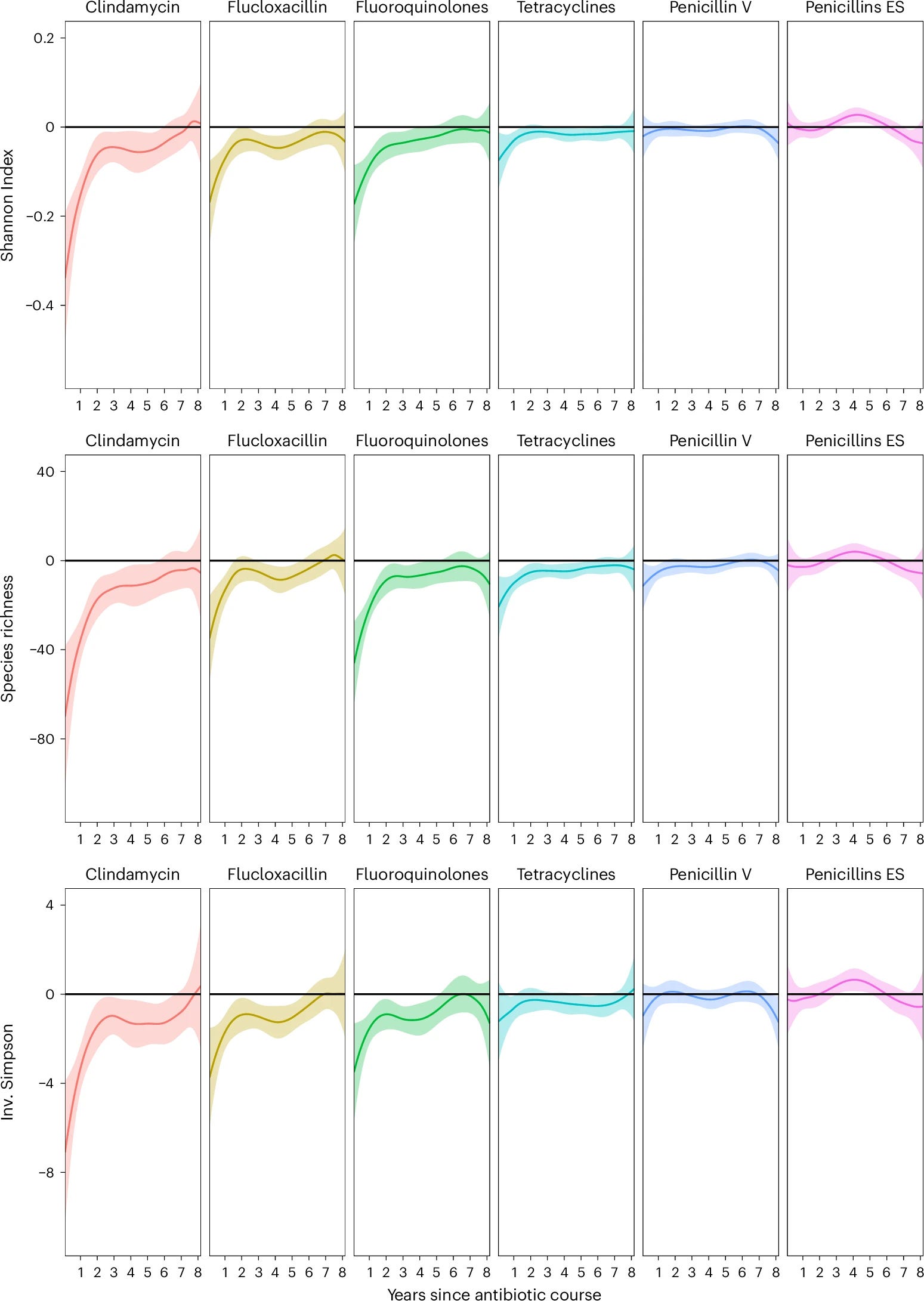
Most of you reading this are aware the gut microbiome is implicated across the entirety of human health: from digestion, immunity, inflammation, and metabolism, to endocrine signaling, brain and mood function, cardiovascular health, susceptibility to infection — everything. The consequences of fucking up our biomes due to monstrous changes in our modern environments, pesticides, and the overuse of antibiotics (agriculturally and clinically) are profound and still poorly characterized. While doxycycline is much less disruptive than some other antibiotics, another reason to consider prophylaxis if you meet all 5 high-risk criteria is the data indicate a single dose has negligible microbiome interruption, while a 10-14 day course, to state the obvious, is much more disruptive.10 We have data on this. Doxycycline is in an antibiotic class called tetracyclines — look at the data below to see that full reconstitution takes years.
The above data are from full antibiotic courses. But the Lyme prophylaxis is a single 200 mg dose. The closest high-resolution human data come from doxy-PEP, where participants took repeated but intermittent 200 mg doses over six months. Even with a median of 42 doses, investigators found no significant residual change in gut microbiome at six months.11 While there are limits to this analysis12, we can say with reasonable confidence that a single prophylactic dose isn’t terribly disturbing to gross gut microbiome composition, certainly not compared to a full course.
We must return again to the task of holding two truths: microbiome function and disruption play a significant and under appreciated role in health and disease, and untreated disseminated Lyme is a much worse problem than a doxycycline-altered gut microbiome.
So avoid ticks if you can. Consider low-risk high-reward prophylaxis if you find a high-risk tick bite. And — while having to take antibiotics sucks — uncontrolled Lyme disease is much worse. More about post-antibiotic biome stewardship later on below.
Treating Lyme Disease
If you are fortunate enough to recognize Lyme disease only after it’s already full-blown, the remaining question I’m exploring — through a cost-benefit lens — is how to approach Lyme disease using a combination of conventional and less conventional treatments, grounded, at least directionally, in an evidence base, to maximally minimize all the awful fat-tail risks.
A note on cost-benefit trade-offs: this is the central question in all of medicine. Every intervention carries its own balance, and this is what guides decision-making. For each person, and every treatment, that balance will differ.
I speak more elsewhere about the epistemology of supplements, herbs, and simple nutritional compounds. But briefly: I’ll be discussing a number of herbs here that do not — and will never — have large, multi-site, double blind randomized placebo-controlled trials.
Is that because they don’t work? No, not necessarily, though we are less certain of how well they work.
Here, the large trials don’t exist because the truth-seeking structures of the biomedical industrial complex require, for those kinds of multimillion-dollar trials, a profit motive — something patentable. And a healing corpus that is limited to treatments that fit within the narrow confines of that structure is a sad corpus. So we need to broaden our epistemology.
Most of these herbs have been used for hundreds, if not thousands of years across multiple traditions. The real-world sample size is enormous, and in most cases, the safety profiles for a time-limited courses is phenomenal — often limited to some GI upset, which is a possibility with nearly anything. (There are always caveats, which is why this is not medical advice. Talk to your doctor, especially if pregnant or with pre-existing medical conditions).
Are the herbs cheap? Not especially. Are they extraordinarily expensive? No. Each herb somewhere between $10 to $30 a month. For someone at the poverty line, this matters more. But for the likely reader with some disposable income, the cost is negligible.
I say all of this to clarify my own stance: for me, the cost-benefit trade-off — of spending a few hundred dollars and risking some GI upset for a marginal increase (at worst) and a substantial increase (at best) in the likelihood of eradicating Lyme — was and is extremely worth it.
I’ll go into more detail about the scientific rational for this approach in a moment. We won’t discuss here all the supportive measures – from rest and nutrition, to time outdoors in nature bathed in copious amounts of infrared light, etc. Those are generalized measures that go without saying. This is about Lyme specifically.
I’ll give credit to a niche independent researcher who turned me on to two research studies, and more credit to Stephen Buhner, an herbalist whose books on Lyme and co-infections were way ahead of the curve in terms of incorporating bioactive herbs and nutraceuticals.
The papers that influenced my thinking here are laboratory studies of Borrelia burgdorferi (the bacterium that causes Lyme disease) and related tick-borne pathogens. The researchers grew the organism in culture and tested how botanical extracts, nutraceuticals, and conventional agents performed against different morphologic states, including actively growing spirochetes, stationary or persister forms, and biofilm-like aggregates. One paper directly screens a panel of botanical medicines against growing and non-growing B. burgdorferi and follows the strongest signals with subculture experiments.13 The other paper surveys a broader literature on botanicals and nutraceuticals studied across Borrelia, Babesia, and Bartonella (common co-infections, often missed) with an emphasis on antimicrobial activity, persistence biology, and biofilm-related mechanisms.14
What’s important here is this helps validate and prioritize, mechanistically, a suite of herbs long utilized in herbalist contexts. Some show activity against forms that are plausibly harder to eradicate — even by doxycycline. Some have additional literature for other indications that demonstrate strong evidence of crossing the blood brain barrier15, and numerous supportive homeostatic-promoting effects. I think it’s reasonable to assume a broad tissue penetration/coverage in totality when utilizing all of them. In short, for a healthy non-pregnant person these are not only safe compounds, but they have a number of health-promoting benefits. And so while we’re not certain about in-vivo activity against Lyme, or human outcome data (and the gulf between Petri dish studies and real life is indeed wide), these are the kinds of compounds that make my cost-benefit decision easy. It creates a rational basis for expanding the toolkit when the downside of a missed or undertreated disseminated infection is high and the downside of a time-limited course of well-chosen herbs is, for me, capped.
Combination Antibiotic + Botanical Approach for Lyme
So the problem is that while a course of Doxy is usually sufficient, it isn’t always. AN under appreciated fact about Borrelia burgdorferi is that it exists in at least three morphologic forms in humans, all with differing susceptibility to different antimicrobial agents. And it is a tricky immune-evasive son of a bitch. Once Lyme reaches immune privileged sites like the central nervous system and joints, drug exposure and clearance become more inconsistent. The approach is to cover a broader and longer array so we are not treating only one form while the others persist.
MY APPROACH:
Start with the antibiotic backbone. Then cover the organism’s phenotype diversity with extracts and do this far beyond the end of the antibiotic course. Unlike doxy, these aren’t going to nuke your gut microbiome, so while there are no human clinical trials for these herbs against Lyme specifically, from the papers and the rational above the cost/benefit here is strongly in favor of a pluralistic approach. Throw the fucking warchest at ‘em. In herbalism folks often start low and titrate over weeks. I chose not to do that. I started seven to nine agents at full dose on day one, about 30 drops two to three times daily for each tincture, i.e. not to fuck around. This was especially true in my case where the fuckers were getting into my facial nerves. DIE.
There are some distinct differences, but also similarities to this herbal approach when thinking about the combination-drug approach to chemotherapy: multiple agents at once, at a kind of maximum tolerated dose, targeting different molecular pathways, likely with different tissue penetrance, and being especially good at various morphologic forms. The main difference is that chemotherapy agents usually rely on therapeutic effects that are inseparable from systemic toxicity, whereas these herbs combine direct antimicrobial activity with systemic immunomodulatory, anti-inflammatory and cytoprotective effects — they support systemic physiology while also killing Lyme. We love that difference.
Again, the fair critique here is the Petri-dish-to-human-outcome gulf. But against the asymmetric risk laid out above — devastating downside of incomplete treatment, modest cost, well-tolerated, health promoting agents — made the decision for my case easy.
ANTIBIOTIC BACKBONE
Doxycycline dosed per evidence based guidelines (ie ask your doctor, course length may differ depending on a number of variables)
Notes on microbiome recovery:
A 2018 paper in Cell found that, after antibiotics, a standard multi-strain probiotic supplement impaired microbiome reconstitution following antibiotic course. This makes sense in a way — probiotics are blunt tools not optimized to your microbiome, and I could speculate blunt forcing of a not-native species makeup crowds your own gut ecosystem as it tries to repopulate on its own. All to say, I do not think post-antibiotic probiotics supplements are a good idea. A healthy mix of whole foods prebiotic plant fibers and dietary probiotics (kefir, yogurt, etc) makes more sense.16
In a future world we’ll have healthy samples of our own stool sitting at a cool -80°C so we can follow the doxy with an autologous fecal transplant to immediately repopulate our gut microbiome but in the event you haven’t already done that prior to antibiotic administration you can skip this step. (The same study from the previous paragraph showed immediate gut recovery after, essentially, eating freeze dried capsules of your own pre-antibiotic shit. Remember: there are levels to the mad scientist biohacking game).17
CORE BOTANICALS FOR LYME DISEASE
If I could only use two I would use these two, which have shown the highest antimicrobial activity in the literature:
Cryptolepis (Cryptolepis): anchor for growing and stationary forms. This is a West African indoloquinone traditionally used for its anti-malaria and broad antibacterial activity against other febrile illnesses.18
Japanese knotweed (Polygonum cuspidatum): resveratrol-rich, pairs well with cryptolepis. A plant native to East Asia, now invasive and abundant in the Northeast US.
Then I layer the rest to span forms and likely niches:
Cat’s Claw (Uncaria tomentosa): persister activity, broad benefits, well tolerated.
Chinese Skullcap (Scutellaria baicalensis): active across forms, calming, often given later in the day.
Wormwood (Artemisia annua): strong activity against stationary phase in vitro, useful when symptoms suggest deeper or coinfection overlap.
Black Walnut (Juglans nigra): bacteriostatic against log phase and bactericidal against round bodies in vitro, screen for nut sensitivity.
Teasel (Dipsacus spp.): optional and traditional. I do not rely on it here.
HOST SUPPORT These are not here to kill B. burgdorferi . Their role is supporting the milieu so killing agents can work while limiting collateral inflammation and preserving competent defense.
Astragalus (Astragalus membranaceus): helps restore innate and adaptive tone, supports dendritic cells and macrophages, supports NK activity, promotes Th balance.
Andrographis (Andrographis paniculata): calms an overactive cytokine environment, downshifts NF kappa B and Th17, may be useful when joints or neuro irritability are an issue.
Mushroom trio: Reishi, Chaga, Lion’s Mane for extra neuroimmune support and recovery
PERSISTER AND BIOFILM INTENSIFIERS I would consider this when disease is severe, dissemination is obvious, or neuro involvement is likely.
Oregano Oil (standardized to carvacrol, Origanum vulgare): hits stationary and biofilm like aggregates and also log phase via carvacrol. Lipophilic with evidence of central penetration. Would prefer enteric or emulsified capsules.
Rockrose (Cistus incanus or Cistus creticus): persister and biofilm support.
Garlic oil with meaningful allicin yield
DURATION – Aggressive phase for 8 to 12 weeks (all herbs). Consolidation for 4 to 6 weeks after symptom resolution. During consolidation I kept Cryptolepis and Japanese knotweed and tapered the others. This was for my early disseminated case with neuro-involvement. There is obviously not an evidence base for the protocol length, but severity should reasonably inform duration.
MINIMAL VIABLE STACK
Cryptolepis (Cryptolepis sanguinolenta) and Japanese knotweed (Polygonum cuspidatum) as anchors.
Add Chinese skullcap (Scutellaria baicalensis), sweet wormwood (Artemisia annua), and cat’s claw (Uncaria tomentosa), +/- astragalus (Astragalus membranaceus) as background support.
If neuro involvement is prominent, keep a lipophilic agent with likely central penetration through consolidation phase, i.e. often oregano oil (Origanum vulgare)
SOURCING AND SUPPLIERS
Many of these are common and available at co-ops and health food stores. If you’re suddenly suspecting an infection, time is of the essence, so if it were me I would start with whatever’s closest. Cryptolepis is the one youre less likely to find locally.
Green Dragon Botanicals carries the hard-to-find and core items, particularly Cryptolepis. They also carry Japanese knotweed (regionally reasonably available in the NE), Andrographis (common), Astragalus (common), cat’s claw (common), skullcap (common), and teasel (kind of common). While of course I can’t vouch for purity, ingredient testing, or contaminants, this source was recommended by an herbalist I trust and was one of my go to suppliers.
Mountain Rose Herbs carries Wormwood (Artemisia annua) and black walnut (Juglans nigra) which are not typically available at Green Dragon. This is a reputable company out of Oregon with an enormous catalogue.
If I was just diagnosed or worrying about Lyme Disease, I would grab what is available now at a nearby health store to get started, then priority ship the remaining items from the suppliers above.
I think it’s reasonable to keep some of these herbs on hand in your home pharmacopeia. If you are worried about a tick bite, fast action can make an enormous difference and its reasonable to hypothesize immediate use of a handful of the most effective herbs — compounds with little downside — may blunt or eliminate any early replicating threat while you consider and/or obtain antibiotics. A medicine cabinet with Cryptolepis and Japanese knotweed would go a long way, adding Chinese skullcap, wormwood, and cat’s claw would round it out well (these herbs have many other uses, too).
I’ll reiterate that my stance is not an either/or, but a yes/and. For my case using conventional treatment and evidence guided herbs made sense. One could imagine a range of scenarios where various mixes of the above are best. Lyme disease is no joke, so try to prevent it, and reach out to a competent physician if you find yourself with a raging infection.
I thankfully recovered well with no residual symptoms. The facial palsy started retreating immediately after implementing everything at once. Thank god.
Remember: this is not medical advice. That said, feel free to ask general questions in the comments.
Cover image: from Bunter Atlas der Pilze und Heilkräuter, c. 1910. Public domain.
This Iwasaki-led review formalized the “post-acute infection syndrome” framework, grouping post-treatment Lyme with long COVID, post-EBV ME/CFS, post-Q-fever fatigue, post-dengue, post-giardiasis, and others, arguing that shared immune dysregulation, dysautonomia, and neuroinflammatory features point to host-mediated rather than pathogen-mediated mechanisms. Choutka J, Jansari V, Hornig M, Iwasaki A. “Unexplained Post-Acute Infection Syndromes,” Nature Medicine 28, no. 5 (2022): 911–923. doi
This Johns Hopkins prospective cohort followed ideally-treated early Lyme patients and found a 13.7% rate of meeting operationalized post-treatment Lyme disease criteria at 6 months, versus 4.1% in controls — a 5.28-fold increase, with the strongest signals in moderate-to-severe fatigue and muscle pain. Aucott JN, Yang T, Yoon I, et al. “Risk of Post-Treatment Lyme Disease in Patients With Ideally-Treated Early Lyme Disease: A Prospective Cohort Study,” International Journal of Infectious Diseases 116 (2022): 230–237. doi
The persistence question splits along two axes. On one side, persistent active Borrelia burgdorferi infection has not been convincingly demonstrated in humans with post-treatment Lyme disease, and the conventional position holds that residual microbial antigens or fragments (rather than living organisms) drive ongoing immune activation, paralleling viral persistence in immune sanctuaries and reactivation of latent herpesviruses (EBV, HHV-6) implicated in both long COVID and ME/CFS.[Kullberg] On the other, B. burgdorferi demonstrably exists in multiple morphologic states — actively growing spirochetes, stationary-phase persisters, and biofilm-like aggregates — with the latter forms surviving antibiotic exposure in vitro and exhibiting reduced metabolic activity that plausibly enables immune and antimicrobial evasion. Whether this in vitro persistence translates to clinically meaningful in vivo persistence in humans remains contested, but the persister biology itself is not in dispute.[Feng] Citations: Kullberg BJ, Vrijmoeth HD, van de Schoor F, Hovius JW. “Lyme Borreliosis: Diagnosis and Management,” BMJ 369 (2020): m1041. doi; Feng J, Leone J, Schweig S, Zhang Y. “Evaluation of Natural and Botanical Medicines for Activity Against Growing and Non-growing Forms of B. burgdorferi,” Frontiers in Medicine 7 (2020): 6. doi
We should note that the CDC does not recommend making treatment decisions based on tick testing because (1) lab quality is variable, (2) a positive tick does not mean it transmitted the infection, and (3) a negative test can falsely reassure you (i.e. a false negative). Nonetheless I have reasonable confidence in the UNH lab linked above, and this may or may not be one relevant piece of date for future treatment decisions — you’ll obviously have to make a prophylaxis decision if it meets high risk criteria before results come back (discussed later in the main text), and a longer course shouldn’t be initiated unless you’re symptomatic and/or serologically confirmed and under the guidance of a physician. But it may provide some worth while reassurance if the result is negative, the tick was found early, and the odds of transmission are low but you’re stressed to the nines catastrophizing (as one does).
This guideline defines which Ixodes bites qualify as high risk and when prophylactic doxycycline is recommended: Lantos et al., “Clinical Practice Guidelines … Lyme Disease,” Clin Infect Dis 72, no. 1 (2021): e1–e48, doi
This review notes that most recognized tick bites are removed before 48 hours, whereas unnoticed bites are more likely to remain attached long enough to transmit Lyme: Shapiro, “Lyme Disease,” N Engl J Med 370, no. 18 (2014): 1724–1731, doi
This Lancet review aggregates persistence-of-symptom data across U.S. and European treatment trials, finding that roughly 11.5% of U.S. and 15.4% of European patients report nonspecific symptoms — fatigue, musculoskeletal pain, cognitive complaints — at six months or longer post-treatment. Stanek G, Wormser GP, Gray J, Strle F. “Lyme Borreliosis,” Lancet 379, no. 9814 (2012): 461–73. doi
This Norwegian RCT comparing oral doxycycline to IV ceftriaxone for European Lyme neuroborreliosis established their equivalence and reported the long tail of residual symptoms — headache, fatigue, cognitive complaints — that persists in a substantial fraction of patients well after antibiotic treatment ends. Ljøstad U, Skogvoll E, Eikeland R, et al. “Oral Doxycycline Versus Intravenous Ceftriaxone for European Lyme Neuroborreliosis: A Multicentre, Non-Inferiority, Double-Blind, Randomised Trial,” Lancet Neurology 7, no. 8 (2008): 690–5. doi
This systematic review pooled 44 LNB studies — including 8 RCTs — with follow-up out to 20 years, finding a weighted mean of 28% of patients (95% CI 23–34%) reporting residual symptoms at latest follow-up. Dersch R, Sommer H, Rauer S, Meerpohl JJ. "Prevalence and Spectrum of Residual Symptoms in Lyme Neuroborreliosis After Pharmacological Treatment: A Systematic Review," Journal of Neurology 263, no. 1 (2016): 17–24. doi
Antibiotics differ in their effects on the gut microbiome: Vich Vila A, Collij V, Sanna S, et al. Impact of commonly used drugs on the composition and metabolic function of the gut microbiota. Nature Communications. 2020;11:362. doi
Repeated single dose 200 mg doxycycline exposure over six months did not meaningfully alter overall gut microbiome diversity or composition (as measured by alpha diversity, beta diversity, taxonomic composition, or bacterial mass) but did increase tetracycline resistance gene abundance and expression in a dose-dependent manner: Chu VT, Glascock A, Donnell D, et al. Impact of doxycycline post-exposure prophylaxis for sexually transmitted infections on the gut microbiome and antimicrobial resistome. Nature Medicine. 2025;31:207–217. doi
“No significant microbiome change” does not mean “nothing happened.” The study used DNA metagenomics and RNA metatranscriptomics, which are strong tools, but sampled rectal swabs at baseline and six months. It could miss short-lived shifts after dosing, effects at other body sites, strain-level changes, or functional changes that normalized before sampling. Nonetheless, I think we can confidently say the effects are trivial compared to a 2-week course.
This is the key in vitro screening paper showing that some commonly used botanicals look much more active than others against Borrelia burgdorferi, including stationary/persister forms; notably, Cryptolepis sanguinolenta and Polygonum cuspidatum (Japanese Knotweed) were among the strongest performers. Jing Feng et al., “Evaluation of Natural and Botanical Medicines for Activity Against Growing and Non-growing Forms of B. burgdorferi,” Frontiers in Medicine 7 (2020): 6. doi
This review is useful because it gathers the broader literature on bioactive phytochemicals, nutraceuticals, and micronutrients across Borrelia, Babesia, and Bartonella, giving a more systematic map of the natural compounds being studied for tick-borne illness rather than treating “herbs for Lyme” as a single undifferentiated category. Samuel M. Shor and Sunjya K. Schweig, “The Use of Natural Bioactive Nutraceuticals in the Management of Tick-Borne Illnesses,” Microorganisms 11, no. 7 (2023): 1792. doi
Based on the available data, active constituents from wormwood, Chinese skullcap, Japanese knotweed, and probably Andrographis cross the blood-brain barrier to some meaningful degree. The evidence is thinner but still plausible for cat’s claw, black walnut, and Cryptolepis.
The evidence on post-antibiotic probiotics is a bit conflicted, but the microbiome-level data makes me cautious. As mentioned in the body, supplemental probiotics taken after a course of antibiotics appear to delay reconstitution of the indigenous gut microbiome rather than help it, colonizing mucosal niches that would otherwise be reoccupied by native species. They do reduce antibiotic-associated diarrhea, but that symptomatic benefit may come at the cost of slower ecological recovery. The clinical significance of the tradeoff is incompletely characterized.
Hence the whole-food-first approach. Diverse prebiotic plant fibers (fruits, vegetables, legumes) provide the raw materials that selectively nourish your indigenous bacteria. Naturally fermented foods (yogurt, kefir if you tolerate lactose, kimchi, sauerkraut, miso) deliver live microbial communities in a complex food matrix (which matters) in much greater diversity, so this is different than isolated commercial strains in a capsule. I think it’s reasonable to believe the whole-food route avoids the monoculture-colonization pitfall and supports recovery through ecological means rather than blunt-force seeding.
Perhaps the most compelling finding from the Suez et al. data (which has been independently replicated) is that autologous fecal microbiota transplant (i.e. aFMT) restores the pre-antibiotic microbiome within days. The future I’m pointing at is one where you store your own stool before an antibiotic courses and restore your microbiome immediately afterward. The downstream costs of antibiotic-induced dysbiosis are under-appreciated and under-characterized. C. difficile infection gets most of the attention, but as I mention in the main text our microbiome is implicated in everything.
I will state again clearly that I’m extremely grateful this is a tradeoff we get to make. Antibiotics are extraordinary and one of the most important discoveries/creations humans have made. The side effects of microbiome disruption are side effects we are fortunate to contend with. The alternative — losing a limb to necrotizing soft tissue infection, dying of sepsis, suffering disseminated Lyme — is incomparably worse. Nonetheless, we are well served to give more attention to the tradeoffs, to minimizing risks and maximizing recovery.
A 2018 Cell study directly compared spontaneous recovery, multi-strain probiotics, and autologous fecal microbiota transplant after antibiotics. Autologous FMT rapidly restored the person’s own microbiome, while probiotics delayed recovery of the native stool and mucosal microbiome: Suez et al., “Post-Antibiotic Gut Mucosal Microbiome Reconstitution Is Impaired by Probiotics and Improved by Autologous FMT,” Cell 174, no. 6 (2018): 1406–1423.e16. doi
A review of Cryptolepis sanguinolenta — a West African medicinal root, summarizing its traditional uses, phytochemistry, pharmacology, antimicrobial activity, and toxicology. For the Lyme-specific papers, see footnotes #7 and #8. Osafo N, Mensah KB, Yeboah OK. Phytochemical and Pharmacological Review of Cryptolepis sanguinolenta (Lindl.) Schlechter. Advances in Pharmacological Sciences. 2017;2017:3026370. doi